







Breast cancer is the most common cancer in American women, accounting for approximately 30-32% of all new female cancer cases per year. In 2026, it is expected that there will be more than 320,000 women and over 2,500 men diagnosed with invasive breast cancer along with more than 60,000 cases of non-invasive ductal carcinoma in situ (DCIS).1,2
AAVBC supports early breast cancer screening, with the data reaffirming it as a vital, evidence-based strategy to detect and treat cases prior to clinical progression; it significantly improves treatment outcomes and survival rates.
Mammography, including both 2D and 3D digital breast tomosynthesis, remains the gold standard for routine screening. It is highly effective at detecting lumps and microcalcifications years before they can be felt. For individuals at average risk, current 2025-26 guidelines recommend beginning these screenings at age 40, as finding cancer in its localized stage results in a 5-year relative survival rate of over 99%.3
In addition to mammography, healthcare providers may utilize Clinical Breast Exams (CBE) during routine physicals to identify physical changes or abnormalities. For high-risk populations, such as those with dense breast tissue or known genetic mutations like BRCA1/2, supplemental tools including Breast MRI and ultrasound are employed to increase diagnostic sensitivity. These primary screening tools are collectively responsible for the fact that approximately 66% of breast cancer cases in the United States are currently diagnosed while still localized and highly treatable.4
Below is a summary table of the current U.S. Breast Cancer Screening Guidelines:
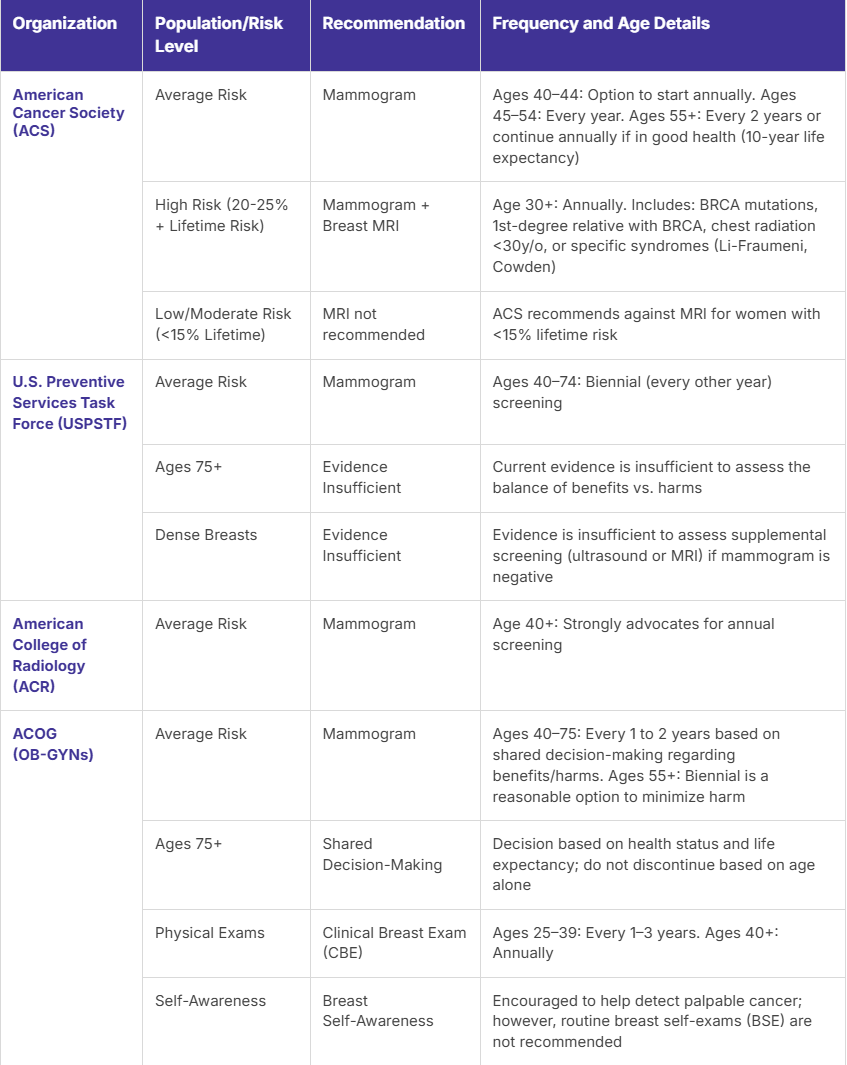
*Lifetime risk scores are calculated using risk assessment tools based on personal and family history. Risk score is often calculated using the Tyrer-Cuzick or Gail Model.
Every patient is different; applying a value-based approach to breast cancer screening requires tailoring your effects to their unique needs and circumstances, such as their risk-level. The following are indicators of a higher-risk patient:
While most organizations agree that screening should begin sometime in your 40s, there are slight variations in the recommended starting age and frequency, highlighting the importance of individualized screening for breast cancer care.
It should be noted that self-exams also play a supporting role in ensuring timely detection. Breast self-examinations (BSE) are recommended monthly for women starting at age 20 so that they can familiarize themselves with their breast tissue, enabling early detection of potential changes. Through this process, a women maintains self-awareness of any changes that should be reported to her physician.
Beyond general guidelines, a proactive approach to identifying high-risk patients is essential to ensure that those with elevated lifetime risks — such as the 20-25% threshold defined by the American Cancer Society (ACS) — receive the intensive surveillance they require. This proactive strategy involves the early application of risk assessment tools like the Tyrer-Cuzick or Gail models to catch individuals who may need to start supplemental MRI and mammography as early as age 30.
Furthermore, the effectiveness of any screening program relies on closed-loop tracking of mammograms. This administrative and clinical safeguard ensures that every ordered test is completed and that results are successfully communicated back to both the provider and the patient. Implementing a closed-loop system minimizes the risk of patients being lost to follow-up, especially when diagnostic imaging reveals abnormalities that require immediate intervention.
AAVBC advocates for a value-based breast cancer screening model focused on prevention, early detection, and seamless continuity of care. We endorse annual mammograms starting at age 40 for women at average risk, with clinical exams and risk-stratified MRI for those at higher risk.
By prioritizing consistent, timely screening, cancer can be detected earlier — improving survival rates and reducing the intensity of treatment. Value-based care in breast cancer screening is not about reducing services. It is about ensuring the right screening occurs at the right time for the right patient, with closed-loop follow-up and shared decision making.
The above content is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions about a medical condition.
