The Medicare Part C (Medicare Advantage, or MA) and Part D (MA-PD) Star Measures program represents the cornerstone of value-based care quality assessment within the Medicare system. It directly impacts over 33 million beneficiaries and determines billions of dollars in quality bonus payments. In 2024, approximately 42% of MA-PD contracts (229 total) earned four stars or higher, and 74% of enrolled beneficiaries were covered under these higher-performing contracts.¹ The Star rating system evaluates Medicare Part C Organizations (Medicare Advantage Organizations, or MAOs) and Prescription Drug Plans (PDPs) across up to 40 distinct quality and performance measures, creating a comprehensive framework for measuring healthcare delivery effectiveness.1
The Star system's evolution reflects CMS's commitment to advancing quality improvement while managing program costs. The average plan Star Rating will decrease from 4.07 to 3.92 in 2025, demonstrating the system's intentional recalibration to continuously raise performance expectations.⁶ Healthcare executives must understand that Star performance directly correlates with financial sustainability, market competitiveness, and regulatory compliance in an increasingly value-driven healthcare environment.
The Medicare Advantage and Part D Star rating system originated from the Medicare Modernization Act of 2003 and the Affordable Care Act of 2010, establishing the first comprehensive quality measurement framework for Medicare managed care.5,6 The program was designed to address three fundamental challenges:
Since the initiation of quality bonus payments in 2012,³,¹¹ the Star system has evolved from a basic performance measurement tool into a comprehensive value-based care framework. After increasing by more than 400% between 2015 and 2023, federal spending on Medicare Advantage bonus payments demonstrates the program's significant growth and financial impact on the healthcare system.³
The Star rating system employs a 5-point scale where higher ratings indicate superior performance:
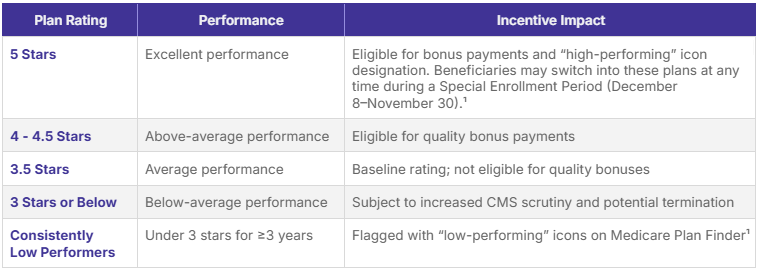
The Centers for Medicare and Medicaid Services (CMS) may terminate a Medicare Advantage plan that fails to achieve a three-Star rating or higher for three consecutive years. Plans consistently scoring below three stars for three years in a row face potential contract non-renewal from CMS. Additionally, CMS issues "consistent poor performer" notices to beneficiaries enrolled in plans with ratings below three stars for three or more years, encouraging them to consider enrolling in higher-quality plans during the Open Enrollment period. This regulatory framework ensures that sustained poor performance has meaningful consequences for plan sponsors.
Organizations that are non-profit more frequently earn higher ratings than organizations that are for-profit. For MA-PDs, approximately 56% of non-profit contracts received 4 or more stars compared to 36% of for-profit MA-PDs, highlighting the correlation between organizational structure and quality outcomes.¹
Star measures operationalize the core principles of value-based care by:
The system creates a comprehensive value equation:
Plan Value = (Quality Outcomes + Patient Experience + Health Equity) ÷ Total Cost of Care
This framework drives healthcare organizations toward population health management, evidence-based care delivery, and patient-centered service models, positioning them for success in value-based contracts beyond Medicare Advantage.
The Centers for Medicare & Medicaid Services (CMS) evaluates Medicare Advantage and Part D plans across five primary Star measure domains: health outcomes, intermediate outcomes, patient experience, access, and process performance. Each domain carries a distinct weight that reflects its contribution to overall plan quality and value-based performance.
Health outcomes measures carry the highest weight in Star calculations, reflecting CMS's emphasis on clinical effectiveness and patient health improvement. These measures evaluate a plans' capacity to deliver care that demonstrably improves beneficiary health status over time.
Health outcomes measures use evidence-based clinical thresholds. Cut-points are recalculated annually using hierarchical clustering with Tukey outlier deletion to ensure statistical validity and minimize distortion from extreme performers.¹,²
Intermediate outcomes focus on clinical quality indicators that serve as proxies for long-term health improvement, emphasizing preventive care and chronic disease management.
A growing number of plans scored highly on some measures like breast cancer screenings, while more plans scored lower on other measures like colorectal cancer screenings, demonstrating the dynamic nature of quality performance across different clinical areas.²
Patient experience measures, derived from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) surveys, assess beneficiary perceptions of care quality, access, and service delivery.7
CMS will reduce the weight of CAHPS and administrative measures from 4x to 2x. This change shifts the focus slightly away from patient experience and administrative efficiency, prompting payers to balance their efforts across a broader range of clinical and outcomes-based quality measures.8
CMS requires all MA, PDP plans and Part D sponsors with 600 or more enrollees as of July of the previous year to survey a defined sample of their eligible members. Plans must contract with CMS-approved vendors for survey administration to ensure standardization and reliability.9-11
Access measures evaluate plans' ability to provide timely, geographically accessible healthcare services to their enrolled populations. These measures focus on structural capabilities rather than direct clinical outcomes.
Process measures assess healthcare delivery efficiency and adherence to evidence-based care protocols, serving as leading indicators of quality outcomes.
The Star Rating system employs sophisticated statistical methods to ensure equitable, reliable and meaningful performance comparisons across diverse plan populations and geographic markets.¹,² The cut points are recalculated each year based on performance during the measurement period. In 2025, many measure-level cut points rose from 2024 levels, requiring plans to achieve higher absolute scores to maintain or improve their ratings.²
Measures undergo case-mix adjustment for patient demographics, health status, and social risk factors to ensure equitable comparisons across different patient populations and geographic areas.1,2
Star measures utilize relative performance benchmarking, where Star Ratings are determined by comparing each plan's performance to the distribution of all plan performances nationally. This approach ensures that ratings reflect current industry capabilities while driving continuous improvement.¹,²
Historically, more experienced contracts in the MA program tend to achieve higher ratings, illustrating how benchmarking implicitly accounts for organizational maturity and accumulated quality-management expertise.¹
To preserve rating integrity, the Star system incorporates multi-year performance tracking to identify trends, ensure rating stability, and prevent manipulation of short-term performance fluctuations.¹,²
Plans scored a 4.37 on average in 2022, compared to current lower averages, demonstrating the system's evolution toward higher performance standards and the impact of pandemic-era adjustments normalizing.1,3
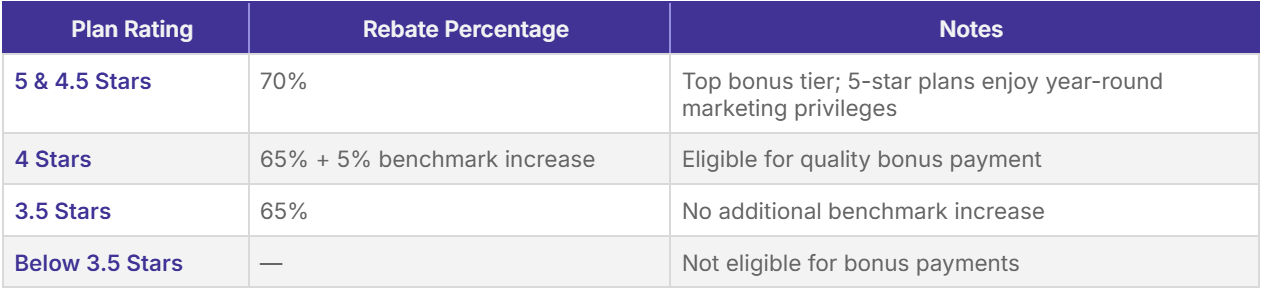
The Quality Bonus Payment (QBP) system represents one of the largest value-based payment programs in healthcare, with substantial financial implications for Medicare Advantage organizations (MAOs). The total spending on the quality bonus program is less than 3% of the projected payments to Medicare Advantage plans in 2024 ($462 billion), yet these payments significantly impact plan profitability and competitive positioning.1,2
UnitedHealthcare receiving the largest total payments ($3.4 billion), and Kaiser Permanente receiving the highest per-member payments, demonstrate how plan size and performance combine to determine total QBP revenue.13
Star ratings shape Medicare Advantage market dynamics far beyond bonus revenue. High-performing plans attract beneficiaries through public visibility on Medicare Plan Finder, enhanced benefit flexibility, and stronger brand reputation.¹,²,⁴,¹⁰,¹¹
Medicare spending on bonus payments has grown faster than enrollment in Medicare Advantage, which doubled between 2015 and 2024 (from 16 million to 33 million people), indicating that quality performance attracts disproportionate enrollment growth.15
Low Star Ratings carry significant financial and regulatory consequences beyond lost bonus payments, including market share erosion, regulatory scrutiny, and increased operational costs.1,2,8
This year's total payouts are a 400+% jump from bonuses back in 2015, when plans got $3 billion total, demonstrating the escalating financial stakes of Star performance in the Medicare Advantage market.16
To illustrate the real-world financial implications, consider a hypothetical 50,000-member Medicare Advantage plan:1,2,5

Successful Star performance requires embedding Star measure requirements into frontline care operations and clinical workflows, while ensuring that care delivery processes naturally generate high-quality outcomes and data capture.1,2,8,9
Organizations should treat Star compliance as core clinical practice rather than an isolated quality project. This includes provider education, workflow redesign, and continuous performance feedback systems tied to measure outcomes and patient experience scores.
Robust data infrastructure forms the foundation of successful Star performance, requiring sophisticated systems for data capture, validation, and reporting across multiple domains.1,2
CPT II codes serve as a critical component of streamlined data collection, enabling real-time performance tracking through claims submission rather than manual chart reviews. These alphanumeric codes significantly reduce administrative burden by automating HEDIS measure reporting, ensuring accurate documentation of clinical activities:
Examples include:
Implementation of CPT II coding protocols facilitates proactive care-gap identification, ensures HEDIS alignment and supports targeted interventions for quality improvement initiatives.12
CMS now requires more frequent data refreshes within Medicare Advantage reporting, shifting organizations toward continuous monitoring rather than annual reviews.²,⁸
Data integrity issues are now included in the description of missing data in the extreme and uncontrollable circumstance (disaster) policy, emphasizing the critical importance of data accuracy and completeness in Star Ratings.¹ Enhanced data validation processes must accommodate more frequent refresh cycles while maintaining accuracy standards for measure calculations and outcome reporting.
Healthcare organizations must develop comprehensive training programs to ensure all staff understand their role in Star performance and quality improvement initiatives.8,9
Top-performing Medicare Advantage organizations align individual goals with organizational Star objectives through incentive programs, recognition, and transparent feedback loops, embedding quality improvement into their operating culture.
Individual providers play a decisive role in determining Medicare Advantage (MA) Star Ratings. Through coordinated clinical practices, patient engagement, and data-driven care delivery, providers can directly influence outcomes, satisfaction, and compliance metrics that determine plan quality scores.¹,²,⁸
These strategies cluster into five operational domains that measurably improve Star performance across preventive, chronic, and experience-based measures.
High-performing providers prioritize strong therapeutic relationships through personalized outreach, education, and continuous communication. This includes using patient-preferred channels (e.g., secure texting, patient portals) and ensuring culturally competent communication tailored to individual needs and language preferences.⁸,⁹
Effective chronic-disease management requires a structured, technology-supported model incorporating remote patient monitoring (RPM) and chronic care management (CCM) programs.
Preventive services directly affect multiple Star categories, including breast cancer screening, colorectal cancer screening, vaccinations, and wellness visits.¹,²
By systematically closing care gaps, providers not only improve clinical outcomes but also raise scores in CAHPS “getting needed care” and “timeliness of care” measures.
Providers should utilize integrated data systems to aggregate member information across care settings, ensuring a comprehensive view of patient health.¹,²
Regular measurement review ensures early course correction and sustained compliance with Star benchmarks.¹,⁸
Care coordination is essential for maintaining high Star scores — particularly for transitions of care, readmissions, and patient-experience measures.¹,²
Formal governance structures and communication protocols should unite clinical, analytic, and operational teams around shared Star objectives.
Star measure success requires coordinated effort across multiple departments and functions, necessitating formal governance structures and communication protocols.
A regional Medicare Advantage plan serving 150,000 members achieved 5-star status through systematic quality improvement initiatives and strategic focus on patient experience.²³
In 2024, 31 MA-PD contracts earned five-star ratings, representing exceptional performance across multiple quality domains.¹
Success required multi-year sustained investment, organizational culture change, and alignment of incentives across all stakeholders. Leadership commitment, continuous measurement, and consistent member engagement were identified as essential for maintaining 5-star performance over successive rating cycles.
A health system-sponsored Medicare Advantage plan integrated Star measure improvement with participation in the Comprehensive Care for Joint Replacement (CJR) bundled-payment program. This alignment establishes a unified model for quality performance across both fee-for-service and Medicare Advantage populations, to create synergistic quality outcomes.8, 17
Independent evaluation of the CJR program showed that 83% of surgeons at participating hospitals reported hospital programs aimed at improving post-discharge care, compared with 47% of surgeons at non-participating hospitals, demonstrating the impact of structured care coordination.¹⁷
The CJR–Star integration demonstrates how bundled payment models and Medicare Advantage quality frameworks can reinforce each other. By sharing infrastructure such as data systems, care coordination staff, and quality dashboards, organizations created positive feedback loops that enhanced quality, lowered costs, and increased beneficiary satisfaction.
The average bonus payment per enrollee is highest for employer- and union-sponsored Medicare Advantage plans ($456) and lowest for special needs plans ($330), raising questions regarding equity within the Quality Bonus Payment (QBP) framework.10,12 Dual-eligible and special-needs populations often present with complex comorbidities, social barriers, and lower baseline quality metrics, making sustained STAR improvement particularly challenging.
A Dual Eligible Special Needs Plan (D-SNP) implemented targeted interventions to address health equity disparities and improve Star performance for vulnerable populations. The program aligned with CMS’s ongoing health-equity strategy, integrating social-determinant interventions with clinical quality workflows.⁷,¹⁰
This case highlights the need for risk adjustment and targeted incentives for MAOs serving high-risk, socioeconomically disadvantaged populations. CMS’s evolving methodology — including the forthcoming Health Equity Index (HEI) adjustment — aims to recognize these challenges while preserving accountability for measurable quality improvement.⁷,¹⁰,¹⁶ Sustained equity-oriented investment within SNPs remains critical to achieving balanced value-based outcomes across the Medicare Advantage landscape.
Sustained excellence in Medicare Advantage Star performance requires a disciplined quality-improvement (QI) infrastructure capable of rapidly testing, validating, and scaling interventions. Leading organizations employ formal methodologies such as Plan-Do-Study-Act (PDSA) and Lean Six Sigma to achieve continuous, evidence-based performance gains.⁸,⁹,1²
Healthcare organizations successful in Star improvement implement systematic quality improvement methodologies that enable rapid testing and scaling of effective interventions. The PDSA cycle enables teams to learn quickly and embed data-driven change into operational workflows without disrupting routine care delivery.
Plan: Identify specific Star measure performance gaps and design targeted interventions.
Do: Implement small-scale pilots with defined populations and timeframes.
Study: Analyze performance data and assess intervention effectiveness.
Act: Scale successful interventions or modify based on learning.
Plan: Implement EHR-based screening reminders for women aged 50-74.
Do: Deploy alerts for 500 eligible members over 3 months.
Study: Analyze screening completion rates and provider satisfaction.
Act: Expand successful reminder system across entire eligible population.
Lean Six Sigma methodologies provide structured approaches to eliminating waste and reducing variation in processes that affect Star measure performance.
Effective Star performance requires advanced population health management (PHM) capabilities that identify, stratify, and proactively intervene with members across the risk spectrum.14,16
By analyzing multiple data sources, predictive models can be used to target specific member populations, increase engagement, and improve overall health outcomes.
Advanced analytics capabilities enable proactive identification of members at risk for poor outcomes and targeted intervention deployment to prevent adverse events.
Successful predictive analytics programs require robust data governance, model validation, workflow integration, and continuous performance monitoring to ensure clinical relevance and operational effectiveness.
Medicare Advantage organizations operate under rigorous CMS oversight and must navigate complex regulatory requirements for Star measure data collection, reporting, and validation to maintain program compliance and avoid penalties.
Organizations must maintain detailed documentation supporting all Star measure submissions, implement approved survey vendor contracts, and respond to CMS information requests within specified timeframes.14
The Star program continues to evolve in response to emerging public-health priorities, technological advancement, and policy initiatives, requiring organizations to plan and prepare for future requirements.
CMS is introducing new measures across several domains, reflecting its desire to address critical areas of patient safety, mental and physical health. It is recommended that providers enable email updates and regularly check for updates and announcements to stay up to date.
CMS will reduce the weight of CAHPS and administrative measures from 4x to 2x. This change shifts the focus slightly away from patient experience and administrative efficiency, prompting payers to balance their efforts across a broader range of quality measures.
Star measures increasingly align with other CMS quality initiatives, creating opportunities for synergistic improvement efforts and coordinated compliance strategies.
Organizations can leverage shared data infrastructure, reporting tools, and improvement initiatives across multiple CMS programs to maximize efficiency and impact.
Healthcare policy experts and industry stakeholders have identified key areas for Star program enhancement and healthcare quality improvement more broadly.
Provider Integration: Strengthen alignment between plan and provider incentives to ensure that clinical practices directly support Star objectives⁸
The Medicare Advantage Star Measures program remains the most comprehensive and financially significant quality measurement system in American healthcare, directly impacting patient care for over 33 million beneficiaries and driving over $11 billion in annual quality-based payments. Health systems and Medicare Advantage Organizations (MAOs), must recognize that Star performance is no longer optional but essential for organizational sustainability and competitive success in the evolving healthcare landscape.
The financial benefits of Star improvement extend far beyond quality bonus payments. High-performing plans achieve:
Quality-based revenue gains are substantial. UnitedHealthcare, for example, received approximately $3.4 billion in 2024 quality-bonus payments, the largest total nationally, highlighting the scale of financial impact achieved through sustained quality leadership.
The Medicare Advantage Star system will continue evolving as healthcare moves toward outcome-based accountability, equity measurement, and technology-enabled quality management. Organizations that treat Star metrics as an extension of their mission — not merely a reporting requirement — will realize durable competitive advantage, improved member health, and greater fiscal stability.
Excellence in Star performance requires transformational change encompassing:
Organizations investing in these competencies will not only achieve superior Star ratings but also lead the transition toward a comprehensive, value-based care ecosystem.
The Star program represents both the present reality and future trajectory of American healthcare quality measurement.. Organizations achieving excellence in Star performance demonstrate the clinical capabilities, operational efficiency, and patient engagement required for success in value-based care across all populations and payment models. The $11.8 billion in quality bonus payments for 2024 represents only the beginning of healthcare's accelerating shift toward comprehensive value-based accountability.
Current Procedural Terminology Category II (CPT II) codes are supplemental tracking codes used primarily to support quality and performance measurement in healthcare, especially within value-based care (VBC) frameworks. Unlike Category I CPT codes, which focus on medical procedures and services, CPT II codes provide additional clinical data for performance evaluation and quality assessment.
CPT II codes are integral to the Healthcare Effectiveness Data and Information Set (HEDIS) measures, supporting the Star Rating system managed by the Centers for Medicare & Medicaid Services (CMS). These codes streamline data collection, enhance clinical documentation accuracy, and improve the efficiency of quality reporting by reducing the need for chart reviews and manual data abstraction.
CPT II codes consist of five characters — four digits followed by the letter 'F.' They categorize clinical data related to:
Using CPT II codes helps providers meet quality benchmarks that directly affect Star ratings, influencing reimbursement, patient care incentives, and provider rankings. Accurate coding supports compliance with CMS performance measures and facilitates proactive care management, improving patient outcomes and organizational efficiency.
The information provided by the American Academy of Value-Based Care (AAVBC) in this overview, including but not limited to Star Measure guidance, and related content, is intended for educational and informational purposes only. This content is designed to assist healthcare providers, organizations, and professionals in understanding and applying Value-Based Care principles, practices, and regulatory compliance standards.
AAVBC does not provide legal, clinical, or medical advice. The content presented should not be interpreted or relied upon as specific legal, medical, clinical, or professional guidance. While efforts are made to ensure the accuracy and currency of the information provided, AAVBC does not guarantee that the materials presented are complete, comprehensive, or without error.
Providers and healthcare professionals must independently evaluate all content and guidance presented herein in the context of applicable laws, regulations, clinical guidelines, payer policies, patient-specific conditions, and contraindications. Any treatments, procedures, diagnostic approaches, medications, or strategies discussed are illustrative and should not be directly applied without a thorough and independent review of current, evidence-based clinical resources, and regulatory requirements.
For coding, documentation, utilization management, quality measures (including STAR ratings), and compliance matters, users are responsible for consulting official guidelines issued by regulatory bodies, including but not limited to the Centers for Medicare & Medicaid Services (CMS), the American Medical Association (AMA), relevant state agencies, and other authoritative entities.
AAVBC expressly disclaims liability for any loss, claim, or damages arising directly or indirectly from the use or reliance on information provided in this document. Users should consult their organization's legal counsel, compliance officer, or qualified professional advisor for advice specific to their situation.
By accessing and using this document, you agree to AAVBC’s terms and acknowledge that the use of the content is at your own risk and discretion.






