









Skin cancer is one of the most common and simultaneously one of the most preventable cancers in the United States, yet it continues to place a substantial burden on patients and the healthcare system. Rising ultraviolet (UV) exposure, aging populations, and inconsistent use of sun protection contribute to steadily increasing incidence rates.
That being said, outcomes are highly dependent on how early lesions are identified and managed – this requires active vigilance from both patients and primary care providers, combined with the appropriate use of existing and emerging skin cancer detection technologies, to achieve the best results.
In this piece, we will discuss the prevalence and impact of skin cancer, who is most at risk, and why early detection meaningfully changes outcomes and healthcare utilization. We will also outline practical prevention strategies and clinical approaches to early identification, including emerging AI-based screening strategies and the role of appropriate biopsy techniques and structured screening in at-risk populations. Finally, we will frame these strategies within a value-based care perspective focused on prevention, efficiency, the careful balance between under- and over-diagnosis, and improved long-term outcomes.
Skin cancer refers to the abnormal growth of skin cells, most commonly caused by ultraviolet (UV) radiation–induced DNA damage. The three most common types are basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and melanoma.
BCC and SCC are collectively referred to as non-melanoma skin cancers and are highly treatable when identified early. Melanoma is less common but more aggressive and accounts for the majority of skin cancer–related deaths.
More than 5 million cases of skin cancer are treated annually in the United States, making it the most common cancer overall.¹ Despite this, it is highly preventable and often curable when detected early.
Skin cancer represents a major and growing public health burden:
Importantly, stage at diagnosis is the strongest predictor of outcome. The 5-year survival rate for localized melanoma is approximately 99%, but drops significantly once regional or distant spread occurs.⁵ Early detection is therefore not only clinically important but also cost-saving.
These misconceptions lead to behavior that decreases adoption of skin cancer prevention strategies or care seeking:
Not adopting effective prevention strategies, and missed or delayed diagnoses ultimately increase downstream healthcare utilization, including more extensive surgical excisions, sentinel lymph node biopsy, systemic immunotherapy, and reconstructive procedures.
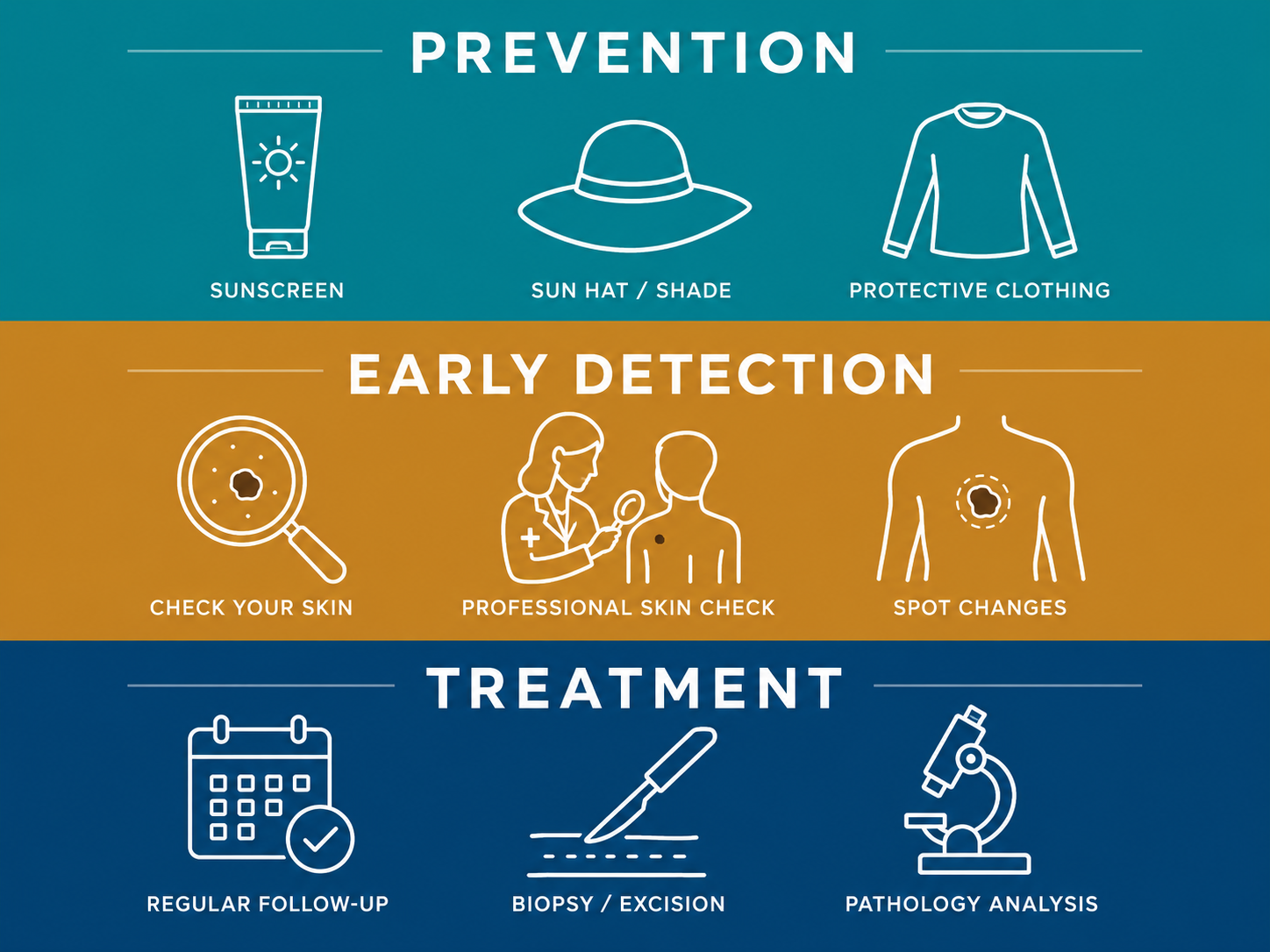
UV exposure is the most modifiable risk factor. Recommended strategies include:
Comprehensive patient education and early detection significantly improves outcomes:
Primary care and dermatology providers play a critical role in thorough skin exams for the early diagnosis of suspicious lesions and follow clinically-grounded biopsy workup:
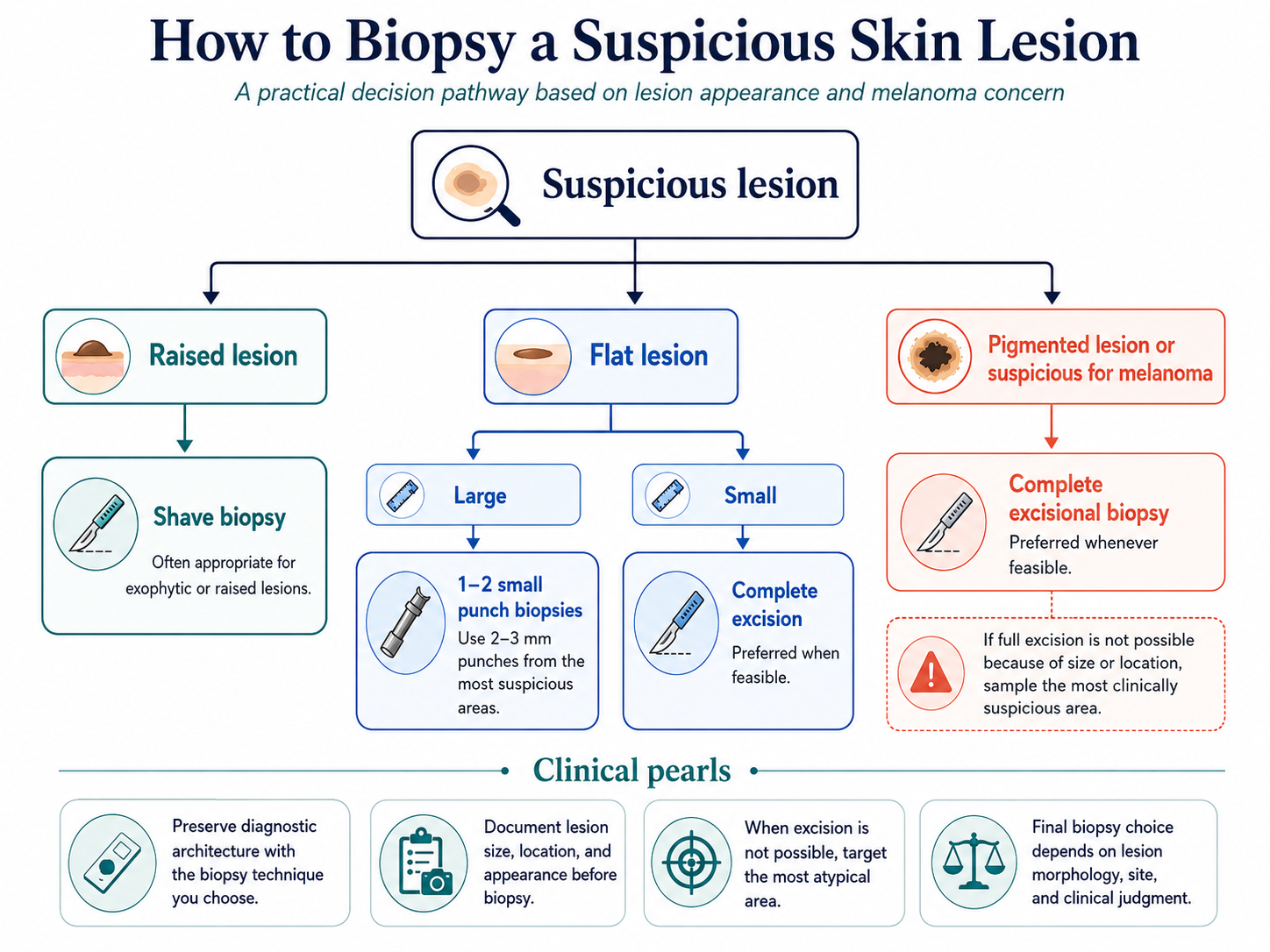
Incorrect biopsy technique can lead to under-staging and delayed definitive treatment, particularly in melanoma where depth of invasion determines prognosis and management.
Surgical excision is the gold standard for confirmed skin cancer, with Mohs micrographic surgery offering the lowest recurrence rates (~1.9%) and maximum tissue conservation, particularly for high-risk or cosmetically sensitive lesions.
Image-Guided Superficial Radiation Therapy (IG-SRT/GentleCure) uses ultrasound-guided superficial radiation to treat NMSC non-invasively, reporting ~99% local control in retrospective studies.
From a value-based care standpoint, skin cancer management is a high-yield area for prevention and early intervention. Early detection reduces:
Emerging AI-based skin surveillance technologies (e.g., smartphone dermoscopy apps, algorithm-assisted lesion tracking) can serve as useful adjuncts for patient-guided monitoring and can support collaboration between patients, PCPs, and dermatologists by flagging concerns about changes in lesions over time. However, these tools are not diagnostic authorities: they do not replace clinical evaluation, dermoscopy by a trained provider, or histopathologic confirmation via biopsy. Their role is best understood as a triage aid that may prompt earlier clinical assessment, not as a substitute for it.
Additionally, accurate documentation and coding of high-risk lesions and precancerous conditions (e.g., actinic keratosis) supports proactive surveillance and population-level risk stratification, enabling a closed-loop referral pathway from screening through diagnosis, treatment, and follow-up.
Skin cancer is one of the most preventable and treatable cancers when identified early, yet it continues to impose a significant clinical and economic burden. Prevention, patient awareness, and timely clinical evaluation remain the most effective tools for improving outcomes.
At AAVBC, we emphasize that skin cancer care is a clear example of value-based medicine in action: prevention, early intervention, accurate coding, and coordinated care pathways directly improve both outcomes and system efficiency.
To learn more about preventive care strategies and chronic disease management approaches, explore additional resources in the AAVBC Knowledge Hub.
The above content is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions about a medical condition.
