









Over the past decade, the clinical conversation about testosterone has shifted. Past concerns centered on cardiovascular risk; today the more pressing question is how readily the therapy can be obtained. Prescriptions are inexpensive, the safety evidence has become more reassuring, and a prescription can now be issued through a brief telehealth encounter.
The trend is evident in the data. U.S. testosterone use more than tripled between 2001 and 2011,1,2 and the number of men receiving treatment rose another 27% between 2018 and 2022.3 Generic injectable formulations cost only a few dollars per dose, and telehealth platforms have replaced what was once a urology referral with a short online intake.10
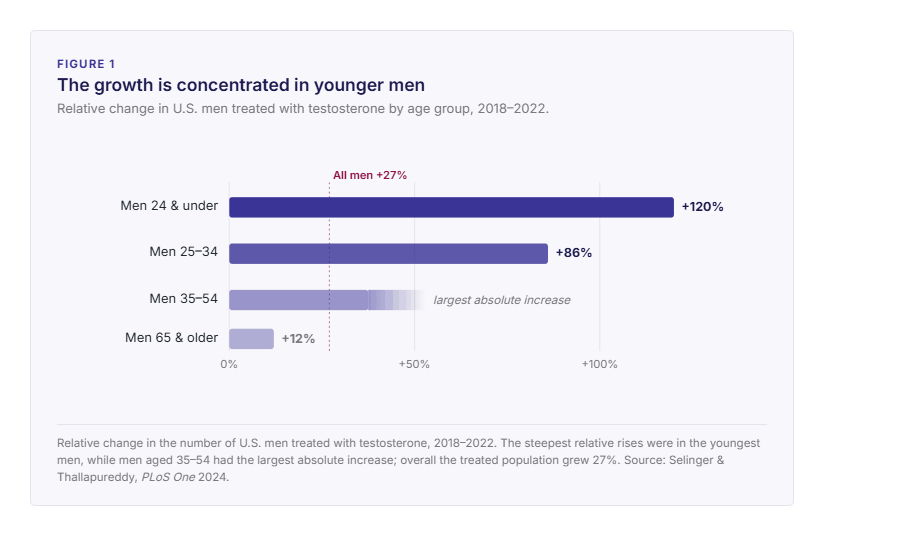
The increase is concentrated among younger men rather than the older patients in whom deficiency is most expected. The steepest relative rises were in the youngest groups, about 120% in men 24 and under and 86% in men 25–34,3 while the largest absolute increases were among men aged 35–54. Many of these patients present with non-specific goals such as improved energy, body composition, or general well-being rather than a confirmed deficiency.
This rise is not without clinical basis. Low testosterone is relatively common, largely because its principal drivers are common: In survey data roughly 1 in 4 adult men have a low level on testing, though far fewer, 1 in 20, have both a low level and the symptoms needed for a diagnosis.11 Prevalence increases with obesity, type 2 diabetes, and poor sleep.
The distinction that matters is between a low number and a confirmed diagnosis, and that is where the clinical work begins.
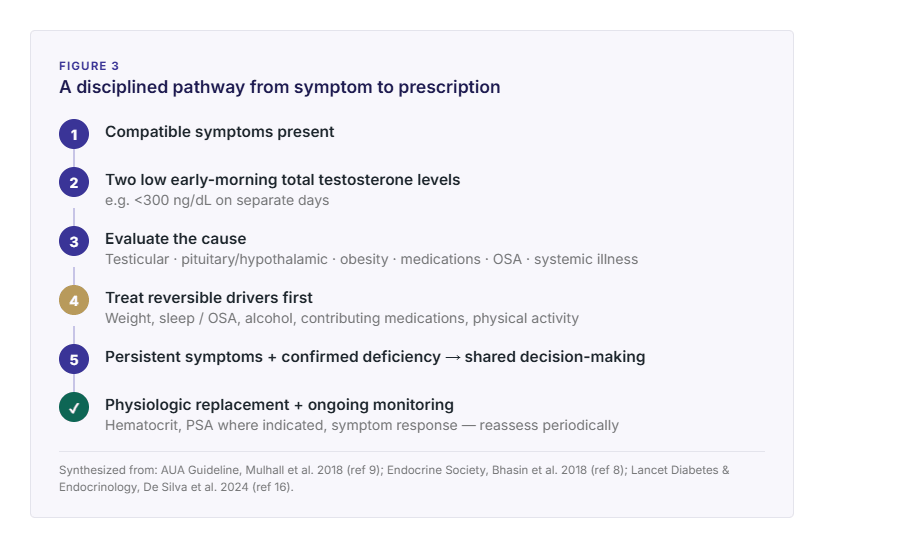
It is a clinical diagnosis, not a single lab value. Three elements have to line up:
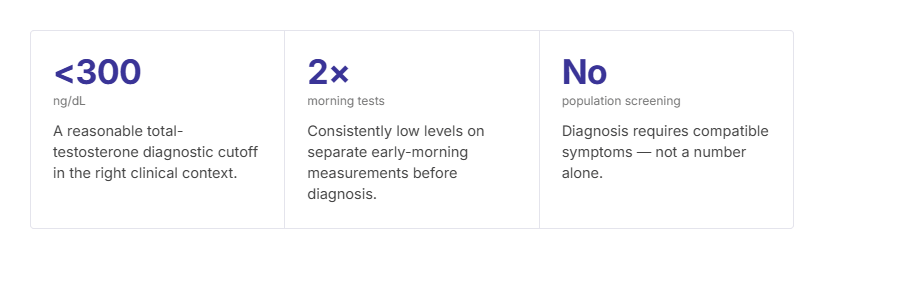
Low testosterone is a clinical diagnosis rather than a single laboratory value, and that distinction is easily lost in expedited prescribing. Three elements must align – compatible symptoms, a total testosterone level consistently below approximately 300 ng/dL, and confirmation on at least two early-morning measurements preferably 2–3 weeks apart, since levels vary across the day and a single afternoon sample can mislead.8,9
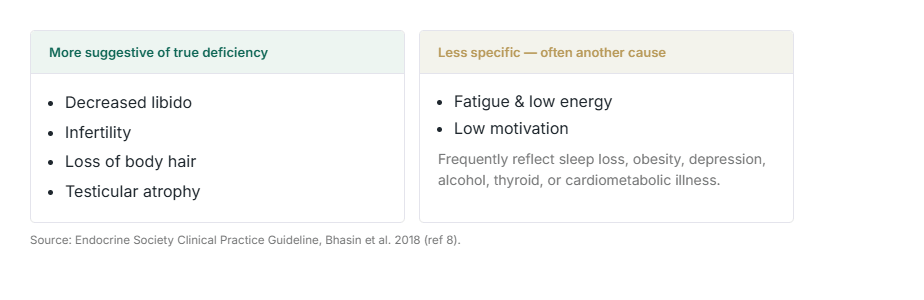
A low result marks the beginning of the evaluation, not its conclusion. The more useful question is why the testosterone level is low. Obesity, untreated obstructive sleep apnea, alcohol use, opioids, type 2 diabetes, and thyroid disease can all suppress testosterone, and several are reversible. The symptoms that most often prompt testing, fatigue and low motivation, are also the least specific, and frequently reflect sleep loss, depression, or cardiometabolic illness rather than a primary hormonal deficit. Omitting this step risks committing a patient to long-term therapy for a condition that weight loss or treatment of sleep apnea might have resolved.
For roughly a decade, cardiovascular concern shaped prescribing. It originated in early observational studies later shown to have methodological limitations, but the resulting boxed warning persisted and discouraged many clinicians.
The TRAVERSE trial addressed much of this uncertainty. It followed 5,246 men with hypogonadism and established or high cardiovascular risk, with a mean treatment duration of about 22 months, and found testosterone non-inferior to placebo for major adverse cardiovascular events.4 On the basis of these results, the FDA removed the cardiovascular boxed warning in 2025.5
These findings are best read with care rather than as a blanket reassurance. The same trial reported higher rates of atrial fibrillation, pulmonary embolism, and acute kidney injury in the testosterone group, and the FDA paired the warning’s removal with a new caution regarding increases in blood pressure.4,5 The reasonable interpretation is that testosterone does not appear to raise the risk of major cardiac events, but it is not without risk and warrants ongoing monitoring.
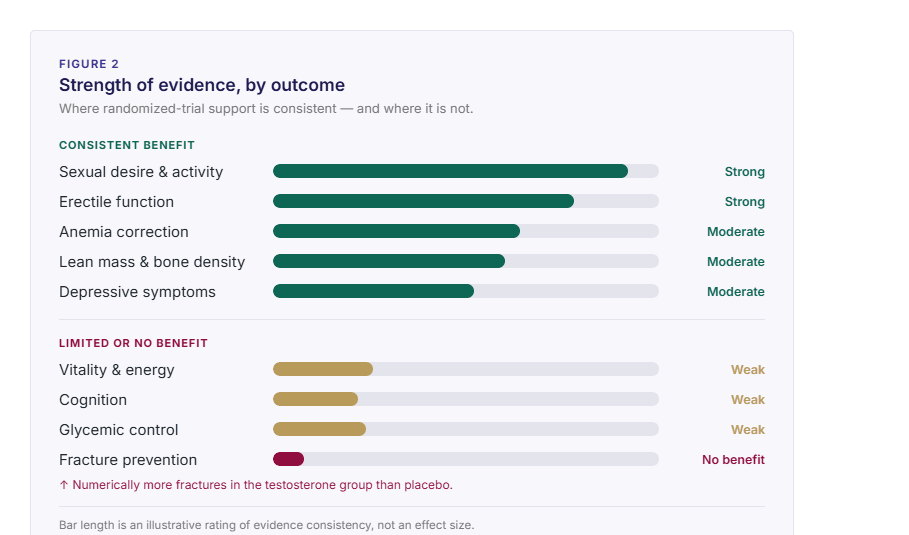
The benefits of testosterone therapy are meaningful but should not be oversold. Across randomized trials, it most consistently improves sexual desire, sexual activity, and erectile function, can improve some depressive symptoms, and can correct anemia and improve lean mass and bone density in hypogonadal men.12,13 The data is much weaker for broad “anti-aging” claims about vitality, cognition, or glycemic control, and the 2024 fracture analysis found no fracture benefit, with numerically more fractures in the testosterone group than placebo.14
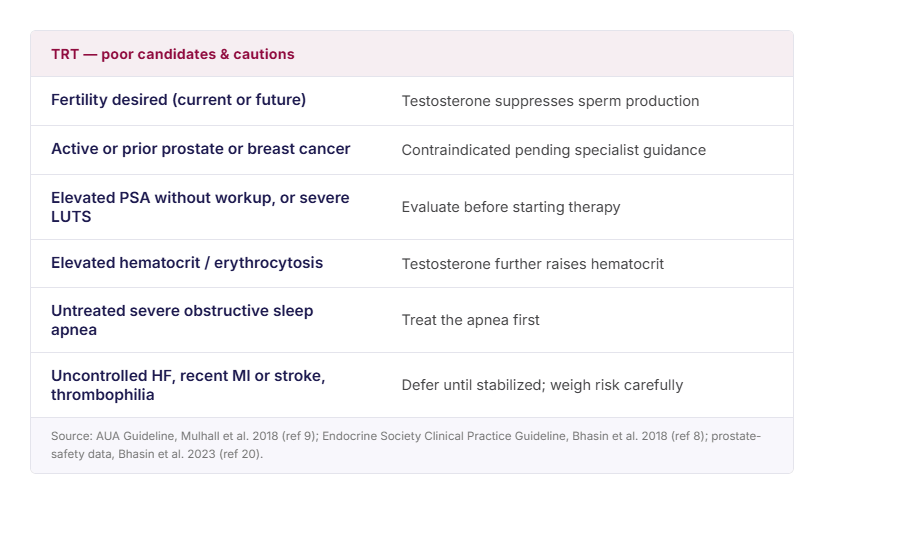
Beyond cardiovascular considerations, several risks merit explicit discussion before therapy begins. The most consequential for younger men is the effect on fertility – exogenous testosterone suppresses and disrupts endogenous production, and most men reach azoospermia or severe oligospermia within three to six months.15 For a patient who hopes to conceive, this is a central consideration, and guidelines advise against initiating testosterone in men who desire fertility within the coming year.8,9
Testosterone also raises hematocrit and can precipitate erythrocytosis; hematocrit is monitored during treatment.8,9 The benefits, while real, are narrower than often portrayed: the evidence is strongest for sexual desire and erectile function, modest for anemia and bone density, and weak or inconsistent for the broader claims of improved mood, energy, cognition, or metabolic control that feature prominently in direct-to-consumer marketing.8,13 The 2024 TRAVERSE fracture analysis found not an absence of benefit but a higher fracture rate in the testosterone group.14 Patients are best served by a clear account of what the therapy can, and cannot, be expected to achieve.
Many men seeking testosterone replacement therapy do not have irreversible gonadal failure. They have functional hypogonadism tied to obesity, type 2 diabetes, poor sleep, chronic stress, alcohol excess, opioids, glucocorticoids, or untreated sleep apnea.16 Obesity is one of the strongest drivers of low testosterone, and substantial weight loss can raise levels and sometimes reverse obesity-related secondary hypogonadism. Sleep pattern and quality are important considerations: even one week of restricted sleep measurably lowers testosterone in healthy young men.17,18
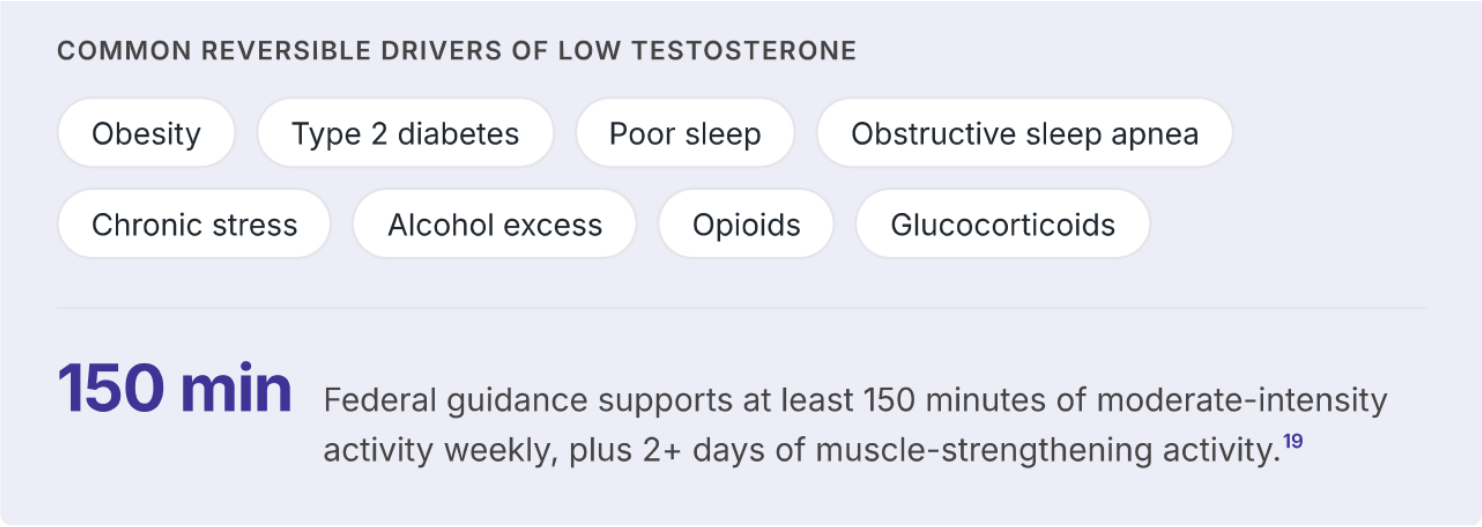
That is why a conservative approach is not dismissive medicine — it is often the highest-value medicine. Before replacing testosterone, many men benefit from improving sleep, screening for sleep apnea, reducing excess adiposity, addressing alcohol and medication contributors, and adding regular physical activity, especially resistance training. Lifestyle change is the only intervention that can improve testosterone while also improving blood pressure, body composition, and long-term cardiometabolic health.
The best primary care candidate is the man with persistent symptoms, two clearly low morning testosterone levels, and an evaluation that supports true hypogonadism rather than a missed reversible driver.8,9 Shared decision-making, not patient demand or boutique branding, should drive the prescription.
Several groups are poor candidates until their underlying issues are addressed:
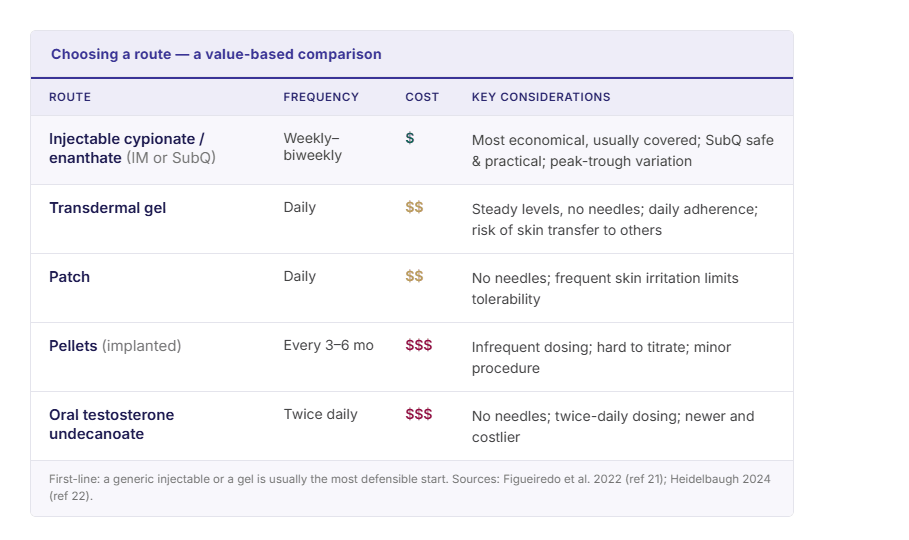
When replacement is appropriate, value-based prescribing means choosing the route that fits the patient’s diagnosis, adherence, monitoring needs, household situation, and cost. For many U.S. patients, generic short-acting injectable testosterone cypionate or enanthate is the most economical and commonly covered option, and subcutaneous self-injection is a safe, practical alternative to intramuscular dosing.21 In practical primary care, a generic injectable or a gel is usually the most defensible first-line start.22
Regulation is moving toward more nuance, not broader prescribing. Alongside the 2025 labeling changes, the FDA in 2026 signaled openness to a possible future indication for low libido in men with idiopathic hypogonadism — an evolving discussion, not a new standard that justifies treating vague aging symptoms.5,23 The goal is not supraphysiologic “optimization.” It is symptom relief with physiologic replacement, ongoing monitoring, and periodic reassessment of whether the therapy is still helping enough to justify its risk and cost.
The above content is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions about a medical condition.
